
Originally By: Khalid Abdulla (edited and modified by FitEyes)
Originally published February 12, 2018
Accuracy and Calibration Of A Goldmann Type Applanation Tonometer
Developed over 50 years ago, goldmann applanation tonometry is often still considered to be the gold standard for the measurement of intraocular pressure (IOP) to this very day.
Please see this related discussion:
Goldmann Applanation Tonometer Calibration Error Frequency | Ask FitEyes
The common misconception among ophthalmologists around goldmann type applanation tonometers is once you have purchased your instrument no routine maintenance or calibration checks are required.
Maintenance is only considered necessary when something has wrong for example:
- The instrument has been dropped and doesn’t work
- The calibration is outside of the original equipment manufacturer (OEM) specification.
The reality is, this assumption is incorrect and there is clinical evidence to suggest regular calibration error checks are required and necessary as route maintenance.
In fact, Wessels and Oh (1990) have also suggested that new tonometers checked within 3 months of purchase may develop calibration errors in the range of 1.5–3.25 mmHg, falling outside the OEM’s acceptable margin of error at ±0.5 mmHg.
Failure to perform routine calibration error checks could ultimately have a negative impact on patient outcomes.
What is the OEM manufacturer’s recommended margin of error?
The OEM recommend calibration error of its goldmann tonometers should remain within ±0.05 mmHg.
Any tonometer found to be outside the margin of error should be removed from clinical practice and returned for recalibration.
What is the current clinical practice for tonometer calibration checks?
A study by Kumar and Hillier published in Eye in 2009 addresses this topic. The purpose of the study was to evaluate the current practice regarding calibration error checks in the United Kingdom and assess the views of senior nursing staff in charge of outpatient clinics as to whom they believe to be responsible for calibration error checks in their department.
Participating ophthalmology units in the UK
A total of 155 eye units were identified in the UK and contacted. A 100% response rate was achieved. All participating facilities used goldmann applanation tonometers in routine clinical practice.
At each institution, a senior nurse familiar with the day-to-day running of the outpatient ophthalmology clinic responded to a structured telephone questionnaire regarding the goldmann tonometer calibrations errors checks.
Respondents were asked how often all goldmann tonometers in clinical practice were checked for calibration errors, and whom they felt to be responsible for checking tonometer’s for calibrations errors (doctor/nurse/departmental responsibility).
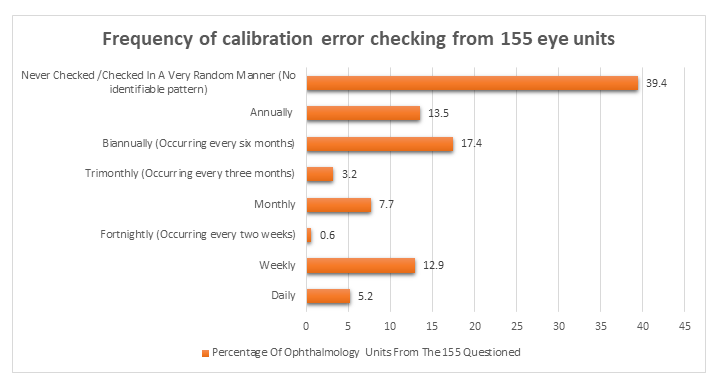
The results:
In 61 Ophthalmology Units, they either ‘Never Checked / Checked in A Very Random Manner’ for calibration errors, representing 39.4% of the 155 units questioned.
In 21 Ophthalmology Units, they ‘Annually’ checked for calibration errors, representing 13.5% of the 155 units questioned.
In 27 Ophthalmology Units, they checked ‘Biannually (every six months)’ for calibration errors, representing 17.4% of the 155 units questioned.
In 5 Ophthalmology Units, they checked ‘Trimonthly (every three months) for calibration errors, representing 3.2% of the 155 units questioned.
12 Ophthalmology Units they checked ‘Monthly’ for calibration errors, representing 7.7% of the 155 units questioned.
1 Ophthalmology Unit checked ‘Fortnightly (every two weeks)’ for calibration errors, representing 0.6% of the 155 units questioned.
20 Ophthalmology Units checked ‘Weekly’ for calibration errors, representing 12.9% of the 155 units questioned.
8 Ophthalmology Units checked ‘Daily’ for calibration errors, representing 5.2% of the 155 units questioned.
Question: Who Is Responsible For Calibration Error Checking?
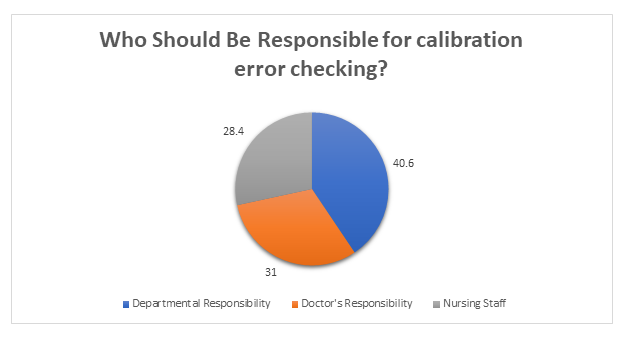
The results:
In 63 Ophthalmology Units, the respondents felt it’s ‘Departmental Responsibility’ to check for calibration errors, representing 40.6% of the 155 units questioned.
In 48 Ophthalmology Units, the respondents felt it’s the ‘Doctor’s Responsibility’ to check for calibration errors, representing 31% of the 155 units questioned.
In 44 Ophthalmology Units, the respondents felt it’s ‘Nursing Staffs’ Responsibility’ to check for calibration errors, representing 28.4% of the 155 units questioned.
How Often should it happen?
The study suggests annual calibration checking is normal practice. However, this is deemed to be insufficient to ensure tonometer accuracy. They suggest that tonometers lose their accuracy during routine clinical practice and may develop calibration error, which frequently over-estimate IOP.
A Doctors Opinion On Who They Felt Calibration Error Checking Lies With
- A previous study by Kumar and Jivan (2007) studied the practice of doctors in the UK and found that 85% of the Doctors surveyed said they have never checked a tonometer for calibration errors and 70% of responding Doctors felt that calibration error checking was not their responsibility.
Verdict: The Doctors believe the responsibility of calibration error checking lies with either nursing staff or other hospital staff to ensure the accuracy of tonometers.
Important Factors This Raises
A previous study by Sandhu et al (2005) aimed to test how many times calibration error checking was required before the error appeared and they found that only 10% of the studied tonometers in clinical use were within the margin of error allowed by the manufacturer of ±0.5 mmHg.
Where Is The Margin Of Error Likely To Show: On The Positive Or Negative Range?
Calibration errors are more likely to show on the positive range rather than negative which may ultimately overestimate IOP measurements. This loss of tonometer accuracy could have a significant impact on a patient's clinical outcome
This Is Great Information, But Again How Does This Help Me And How Does It Answer The Question Of Why An Accurate Tonometer Is Vital For IOP Measurement?
To answer the problem, we must first understand the underlining cause of the problem. Only then can we break down the problem to solve each intricate part one problem at a time.
From the clinical information discussed earlier what is abundantly clear so far is that there is no clear consensus of where the responsibility of calibration error checking lies.
This means that tonometers currently in clinical use may be receiving inadequate calibration error checks.
A study by Turner and colleagues (2013) from Australia including 3654 IOP measurements found that 1mm Hg under or over reading of tonometer will miss 34% of people with ocular hypertension or result in 58% more positive screening tests, respectively. Similarly, a 4mm Hg under or over reading would miss 76% of individuals with ocular hypertension or over-detect seven times more people. This has important implications for clinical care and resources as over-detection could result in more than usual referrals to ophthalmologists, while under-detection may place individuals at higher risk of glaucoma.
Therefore, its vitally important each eye unit develop a directive/procedure to ensure that all tonometer’s in clinical use are given the correct amount of attention to ensure they all meet the adhered to specification outlined by the OEM manufacturer.
What Would Your Recommendation For Privately Owned Optical Practices.
It is vital to keep a ‘Calibration Bar’ handy in each examination room.
Before you open for business, first thing in morning the practice manager or lead optician should first go around all the examination rooms and test each tonometer for any calibration errors and make sure it sits within the OEM manufacturers’ acceptable margin of error at ±0.5 mmHg. (This should take no longer than 3 minutes per tonometer.
Each tonometer should also be tested at all three sequences ‘0’, ‘2’ & ‘6’.
Furthermore, when examining a patient, it is important to double check the instrument you are using functions correctly before using it on a patient. This means performing a quick calibration check on ‘0’ & ‘2’.
How To Check The Calibration Of A Goldmann Type Applanation Tonometer
For full recommendations for medical practices and hospitals, as well as calibration instructions, please see the original article at:
brawnmedical.com/blog/how-check-calibration-goldmann-applanation-tonometer
Closing Comments
It cannot be underestimated as to how important a well calibrated tonometer is vital in the management of glaucoma. IOP is the only medically treatable risk factor for glaucoma. [For the profession to have such a cavalier attitude toward the calibration of the tonometers it typically (and erroneously) refers to as the "gold standard" is shameful.]
Conclusion
Key lessons to take away from this:
- Accurate IOP measurement can only be obtained if the tonometer in question adheres to the OEM guides that allows for a margin of error no greater than ±0.5 mmHg.
- Frequent and Regular Calibration Error Checking in an outpatient or private practice environment is essential to ensure every tonometer in a clinical setting is functioning correctly.
- Calibration Error Checks should be performed before the start of each new clinic day. Any instrument not within the desired specification of ±0.5 mmHg should be remove from clinical use, and returned for a Full Service and NOT just a ‘re-calibration’.
References
Kumar N, Hillier RJ. Goldmann tonometer calibration: a national survey. Eye. 2009 Feb 1;23(2):413.
Sandhu SS, Chattopadhyay S, Birch MK, Ray-Chaudhuri N. Frequency of Goldmann applanation tonometer calibration error checks. Journal of glaucoma. 2005 Jun 1;14(3):215-8.
Kumar N, Jivan S. Goldmann applanation tonometer calibration error checks: current practice in the UK. Eye. 2007 Jun 1;21(6):733.
Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Archives of ophthalmology. 2002 Oct 1;120(10):1268-79.
Turner MJ, Graham SL, Avolio AP, Mitchell P. Potential effects of systematic errors in intraocular pressure measurements on screening for ocular hypertension. Eye. 2013 Apr;27(4):502.
Wessels IF, Oh Y. Tonometer utilization, accuracy, and calibration under field conditions. Archives of ophthalmology. 1990 Dec 1;108(12):1709-12.
Disclaimer: All material reproduced in this article relating to the original clinical publication has been done so with the explicit written consent of the original author (Dr Nishant Kumar (MRCOphth, FRCOphth). Brawn Medical accept no credit for the work undertaken by the original author and acknowledges the full credit goes to the original author of the publication. To access the original publication, you may do so here.
References to OEM goldmann standard of calibration error checking has been done so with widely available material published in the OEM's instruction manual. Images used in this publication are referenced from the Keeler KAT instruction manual.
Acknowledgements: Dr Nishant Kumar (MRCOphth & FRCOphth) Consultant Ophthalmologist & Vitreo-Retinal Surgeon & Uveitis Specialist.