
Abstract
The recent advent of continuous intraocular pressure (IOP) telemetry has led to an increased awareness of the importance of IOP fluctuations, and theories have emerged that IOP variations could play as much a role in glaucoma progression as the mean level of IOP. The aim of the present study was to evaluate the direct effect of common daily activities on IOP-related profiles.
Primary open-angle glaucoma and glaucoma suspect patients were prospectively enrolled from specialist clinics at the University of California San Diego (UCSD), USA. Patients were fitted with a SENSIMED Triggerfish (TF) contact lens sensor (CLS) and were instructed to return to their usual daily activities for 24 h. They were asked to record each specific activity or event in a diary. The protocol was repeated twice.
The following events were recorded:
- “walking/cycling”
- “resistance training”
- “yoga/meditation”
- “emotional stress”
Contact lens sensor measurements recorded 60-to-30 min prior to each event were used as a baseline reference, and all IOP-related fluctuations for 120 min after the start of each event were reported in relation to this reference. Forty relevant events from 22 CLS recordings in 14 patients were retrieved from the diaries.
Walking/cycling (n = 10) caused a small but statistically significant elevation of the IOP-related profile during the activity (p = 0.018).
Resistance training (n = 11) caused a persistent elevation of the IOP-related profile from the onset of the activity (p = 0.005) through 120 min after the activity was stopped (p = 0.007).
Yoga/meditation (n = 4) caused a sustained drop in the IOP-related profiles through to 120 min, although this was not statistically significant (p > 0.380).
Emotional stress (n = 13) was associated with a gradual elevation of the IOP-related profile from the start of the stressful stimulus.
Both early and late variations were statistically significant (p = 0.038 and p = 0.021, respectively).
Images
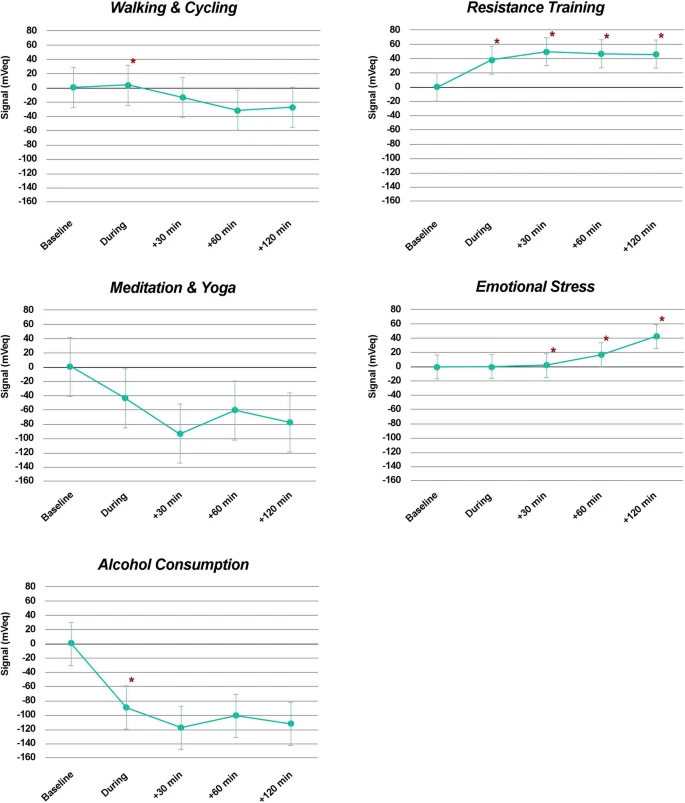
Figure 1: Mean effect of each group of activities on intraocular pressure-related signal recorded in mVeq, during the event, within 30 min of the end of the event, between 30 and 60 min of the end of the event, and between 90 and 120 min of the end of the event, compared to baseline measurements set at 0 mVeq (30–60 min before the start of the event). Vertical bars represent the 95% confidence interval, and asterisks represent statistically significant differences from baseline (p < 0.05).
Discussions
The present study confirms the effect of physical activities, emotional state and alcohol consumption on IOP-related profiles.
Commentary
The sections that follow contain commentary on selected content from the full text scientific publication. If you wish to ask any questions related to this scientific publication, please create a new question. You can reference this FitEyes post in your question.
Limitations Of the Study and General Thoughts
From the article:
This study has several limitations. First, its cohort was relatively small with only 41 eyes and even fewer patients partaking in each activity.
The authors continue to list several other limitations. They also say:
Thus, while caution may be used before generalizing the present results, this study constitutes, as far as we are aware, the first observation of the effect of a range of real-life, non-standardized, daily activities on IOP-related profiles using 24-h continuous contact lens sensor monitoring. Further real-life studies based on larger cohorts to explore the effect of more day-to-day events are warranted.
I am incredibly happy to see glaucoma research looking at real-life IOP as it relates to activities under the patient's control (such as walking, yoga, meditation, stress management, and exercise). This has been the central theme of FitEyes for 15 years.
While FitEyes has not published most of its findings in peer-reviewed journals (yet), I trust the entire body of observations from the FitEyes community more than I trust this limited study. In some cases our findings agree with those published here, and in some cases there is disagreement.
In particular, there is disagreement regarding the effects of weight lifting on IOP.
Weight lifting
The reported results confirm the association between resistance training and IOP elevation that had been previously described by Vera et al. See:
In a study of 25 healthy volunteers, they identified an instant IOP elevation during resistance training that was directly correlated to the intensity of the effort and to the size of the muscle trained. Interestingly, they described a prompt reduction of IOP to baseline within 10 s after the end of muscle contraction, while our measurements suggest prolonged elevation through to 120 min.
The bulk of FitEyes data suggests the following:
Breathing patterns during exercise, amount of intensity and the specific exercise performed all affect IOP during exercise.
My own approach is to warm up gently to avoid increasing my IOP. After just 5 or ten minutes my IOP will be as much as 3-5 mmHg below baseline. Then, during my more intense lifting, the momentary IOP elevation during the lifting does not take my IOP above baseline, as long as I practice good technique (including proper breathing).
In the studies I have seen on glaucoma or intraocular pressure and weight lifting, the researchers have not made any effort to instruct the subjects in best practices.
The bulk of our FitEyes data supports the observation of a prompt reduction in IOP immediately upon the conclusion of the weight lifting effort. Furthermore, we see that working larger muscles (as in the squat exercise) produces larger reductions below baseline than observed when exercising smaller muscles or doing isolation movements (e.g., a bicep curl).
Most importantly, FitEyes data shows that most glaucoma patients see a lasting benefit in reduced intraocular pressure following weight lifting. Sometimes that benefit only lasts 30 minutes. However, it is a common observation that if other factors such as emotional stress were contributing to an elevation of IOP above baseline, weight lifting can eliminate that effect so that one's IOP stays at baseline many hours following the exercise (even for the duration of the day).
However, there are important exceptions. Some FitEyes members have reported that weight lifting increases their IOP, as reported in this study. Therefore, I continue to advocate that every glaucoma patient should have access to a tonometer so they can perform self-tonometry to monitor their own eye pressure in real-life and in real-time.
The present study continues:
This may be explained by differences in methods and measurement techniques. Indeed, while Vera et al. used single groups of 6 rapid consecutive rebound tonometer readings at the start, during and at the end of the exercise period to evaluate its effect, the automated nature of the CLS recording did not permit the matching of recording bursts with specific phases of the exercise. Therefore, we have averaged all the contact lens sensor recordings over 30-min-long periods before and for up to 120 min after resistance training to evaluate any lasting effect. While not movement-synchronized, the 1800 samples recorded during every 30-min period are expected to provide a more faithful representation of the short-term IOP-related fluctuations following each event.
I am skeptical of that claim. Vera et al. used an Icare tonometer. I have personally used both Icare and Reichert tonometers for these weight lifting experiments. Other FitEyes members have used a mixture of both those tonometers.
The contact lens sensor measurements are not performed continuously. The contact lens takes a limited number of measurements during each window of time. Furthermore, if the devices senses that it is generating too much heat during the monitoring process, it stops monitoring temporarily.
I believe it is important to be able to match the IOP measurements with the specific activity or event that was happening at that moment. I do not think the methodology used in this paper is superior, and I suspect it may be inferior to the methodology of Vera et al. and that used by FitEyes members who are rigorous.
Furthermore, the IOP-related profile elevation within the 30 min following resistance training may simply represent the effect of short-term effort-related hormone release. Finally, differences in populations may explain some of the differences observed, since Vera et al. had enrolled healthy young adults, as compared to a population with, on average, older adults with a diagnosis of glaucoma or glaucoma suspect in the present study. Further research will be needed to explore the short- and long-term effects of resistance training on IOP.
Again, I am so happy to see serious glaucoma researchers exploring this topic. Further research is a great suggestion. We can potentially do some of that research in the FitEyes community. However, because there certainly are individual variations, the most important things is not general conclusions coming from this type of research, but knowing specifically how your own individual eye pressure responds to the activities you perform in your own life.
The ultimate answer is that every glaucoma patient needs access to a tonometer they can use at home, in real life and in real-time.
Walking
To the best of our knowledge, the effect of walking or cycling on IOP had not been previously studied.
Here's an article where I discuss walking near the end of the article. It has also been a frequent topic of discussion on FitEyes for the last 15 years.
Doing things slowly in a fast world | FitEyes.com
One of my interesting observations I shared in that article was:
I have the habit of walking in the evenings. Until more recently, I tried to walk fast. I felt like I needed to get the cardio benefits of physical exercise. That immediately led to the idea that the more miles I walked in my given hour of time, the better I was doing.
Soon I discovered that my walks did not always lower my IOP. Eventually, I tried the idea of walking slowly. At first walking slowly was actually psychologically painful. I felt that I was wasting my time. Eventually, I learned to let myself do it and I found that I could consistently produce lower IOP by walking slower. My best walking is when I turn off my thinking brain and just walk as slow and as relaxed as I feel like walking. When I give up on the idea of making it into a productive exercise, I get much lower IOP. Moral of the story: slower is better. ;)
The present study says:
Since the intensity of the activity was not recorded, intense walking or cycling, either uphill or for extended periods of time, might have had the same physiological effect as resistance training.
Participants were not specifically instructed to monitor their fluid intake, which may have a cofounding effect.
In a relatively small cohort, individual variations, whether they be in terms of ocular physiology, hydration, environment, effort intensity or recovery, may have affected the statistical significance of late IOP-related profiles. These reasons might explain the conflicting reports on the effect of regular exercise in the literature.
I agree with most of that. As I said, the speeds and intensity of my own walking does affect how efficacious it is in reducing my IOP. Also, my state of mind plays a part.
The article mentions:
Endurance training was associated with wide variations in plasma levels of a number of [several] neurotransmitters and hormones that may have different effects on the control of IOP.
While researchers sort out all the varying and complex effects of these neurotransmitters and hormones, we can already take some control of our own IOP by learning how to walk in the way that most effectively manages our IOP. We can do that through self-tonometry and experimentation.
The combination of walking, relaxing and letting go of thoughts (being in the moment, simply observing the environment) will have a profound effect on many neurotransmitters and hormones. Without resorting to the reductionistic approach, we can use self-tonometry to optimize the outcome.
Meditation
The present study showed a non-significant drop in IOP-related profile during and after Meditation and yoga. While Jasien et al. demonstrated a marked increase in IOP in all head-down yoga positions evaluated36, large studies concentrating on the effect of meditation defined as simple mindfulness reported a significant persistent IOP-lowering effect associated with the daily practice of the activity for 21 consecutive days37. Thus, the non-significance of our results may be explained (1) by the inclusion of both yoga and meditation within the same analysis, potentially confusing the results depending on the yoga positions practiced by the subjects, (2) by the occasional practice of meditation in the studied subjects, suggesting the importance of daily practice to achieve persistent effect, and (3) by the relatively small number of Meditation and yoga sessions recorded in the present study.
I would add to that the results of my own research on meditation and glaucoma wherein I found that different meditation techniques produce different IOP outcomes.
I believe, in the long run, that a regular meditation practice is one of the most beneficial activities any glaucoma patient can engage in.
However, when first starting a meditation practice, there can be a tendency for IOP to increase after meditation. This effect goes away in time -- provided one is practicing a suitable meditation technique.
While the type of meditation I have been practicing has demonstrated a consistent IOP-lowering effect, one of the most surprising observations related to meditation I have seen was as follows:
A FitEyes member recently acquired a Reichert tonometer. She was a self-taught meditator and she believed her meditation practice was beneficial for her eyes (and glaucoma). Before starting her meditation her IOP was 20 mmHg in each eye. After 30 minutes of meditation, her IOP rose to 40 mmHg!
Without a tonometer, she would never have known this. She would have continued practicing her meditation method believing it was helping when in fact it was harmful. Obviously, I recommended that she learn a new meditation technique -- and learn it from a qualified teacher.
Around the 2008 period, I began a 2 year study on meditation and IOP. As stated, I found that different meditation methods can produce radically different effects on IOP (and heart rhythms, breathing patterns, brain waves, etc.). I was searching for a meditation method that was easy to practice, reduced my stress, improved inner peace and clarity of mind, helped me progress toward equanimity and balanced emotions, improved overall well-being and health and also reduced my IOP. It turns out that fulfilling all those requires proved to be too much to ask of many meditation techniques.
More recently, since early 2019, I have been engaged in further research on meditation and IOP. I am now convinced that we have techniques at our disposal which can profoundly empower us to manage our glaucoma. It is great to see the two words "meditation" and "glaucoma" mentioned together in any serious scientific publication. But what has been reported so far in the scientific literature is a drop in the bucket of what is possible.